
Medical & editorial notice: Symptoms Insight publishes general health information for educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified healthcare provider with questions about a medical condition.
Review snapshot
What we checked for this guide
Official sources used
Pages checked while updating this article
Introduction
Iron deficiency anemia is the most common nutritional deficiency worldwide — and one of the most underdiagnosed causes of chronic tiredness. When your body lacks enough iron to produce healthy red blood cells, oxygen delivery to tissues drops. The result: exhaustion that sleep does not fix, breathlessness on stairs, pale skin, and hair that sheds more than usual.
Iron problems rarely exist in isolation. Fatigue from low iron can look identical to Vitamin B12 deficiency, Vitamin D deficiency, thyroid disorders, or chronic stress. That overlap is why proper blood testing matters before guessing at supplements.
This guide covers iron deficiency symptoms, root causes, how doctors diagnose anemia, evidence-based treatment, the best iron-rich foods, and when symptoms require urgent care. For related nutrient guides, explore our Symptoms & Conditions and Vitamin Deficiency & Nutrition hubs.
Medical note: This article is for general education only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider for personal medical decisions.
What Is Iron Deficiency Anemia?
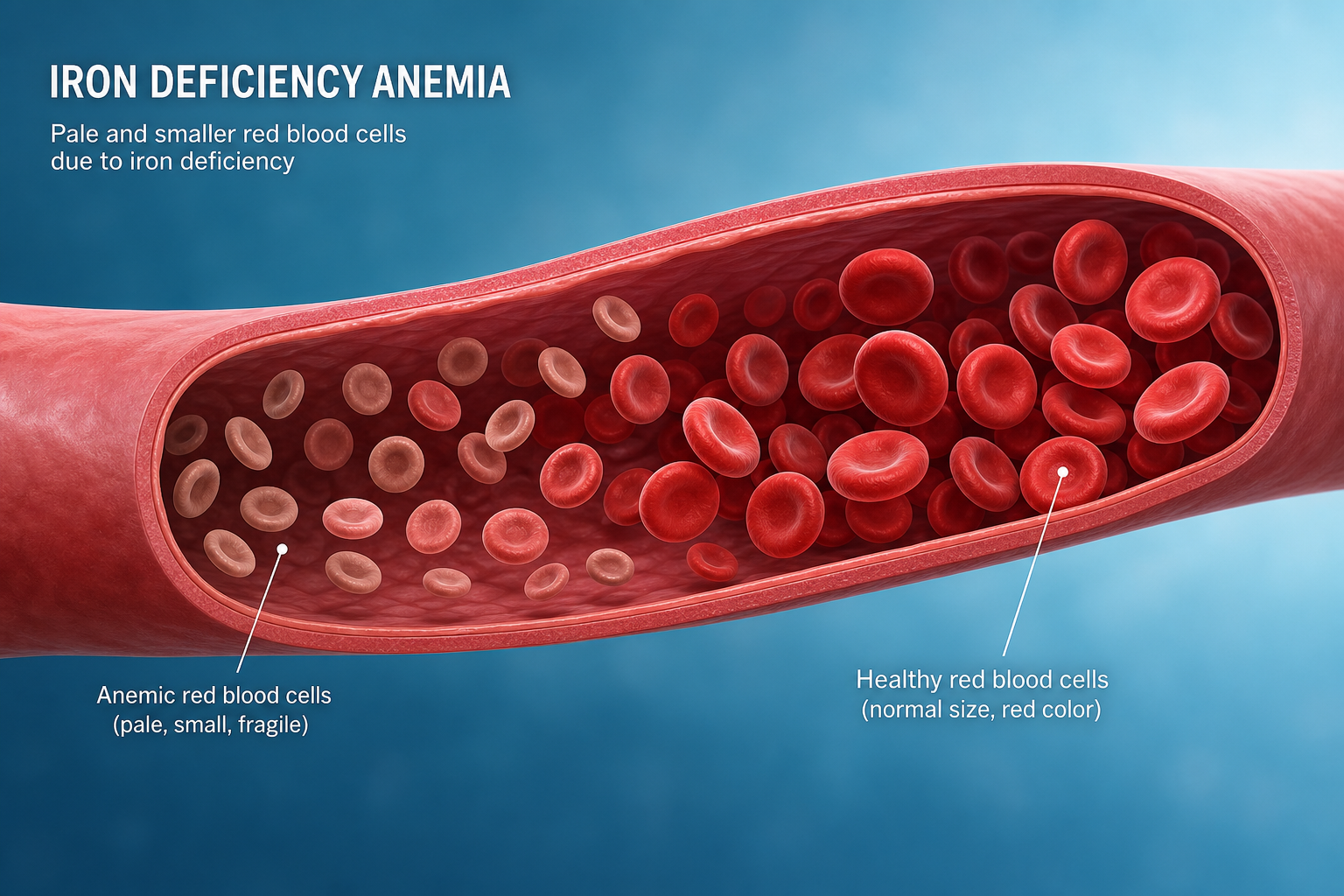
Iron is an essential mineral used to make hemoglobin — the oxygen-carrying protein inside red blood cells. Your body also stores iron as ferritin for future use.
Iron deficiency means iron stores are depleted. Iron deficiency anemia means deficiency has progressed enough to reduce hemoglobin or red blood cell production. According to the World Health Organization, anemia affects roughly one-quarter of the global population, with iron deficiency as the leading cause.
Why iron matters for your body
| Role | What happens when iron is low |
|---|---|
| Oxygen transport | Less hemoglobin → tissues receive less oxygen → fatigue |
| Energy metabolism | Iron supports cellular energy production (ATP) |
| Immune function | Deficiency may impair immune cell activity |
| Brain development | Critical in infants and children for cognition |
| Hair & skin health | Low iron linked to shedding, brittle nails, pale complexion |
| Exercise performance | Reduced endurance and recovery in athletes |
Iron Deficiency Symptoms
Symptoms develop gradually. Many people adapt until deficiency becomes moderate or severe.
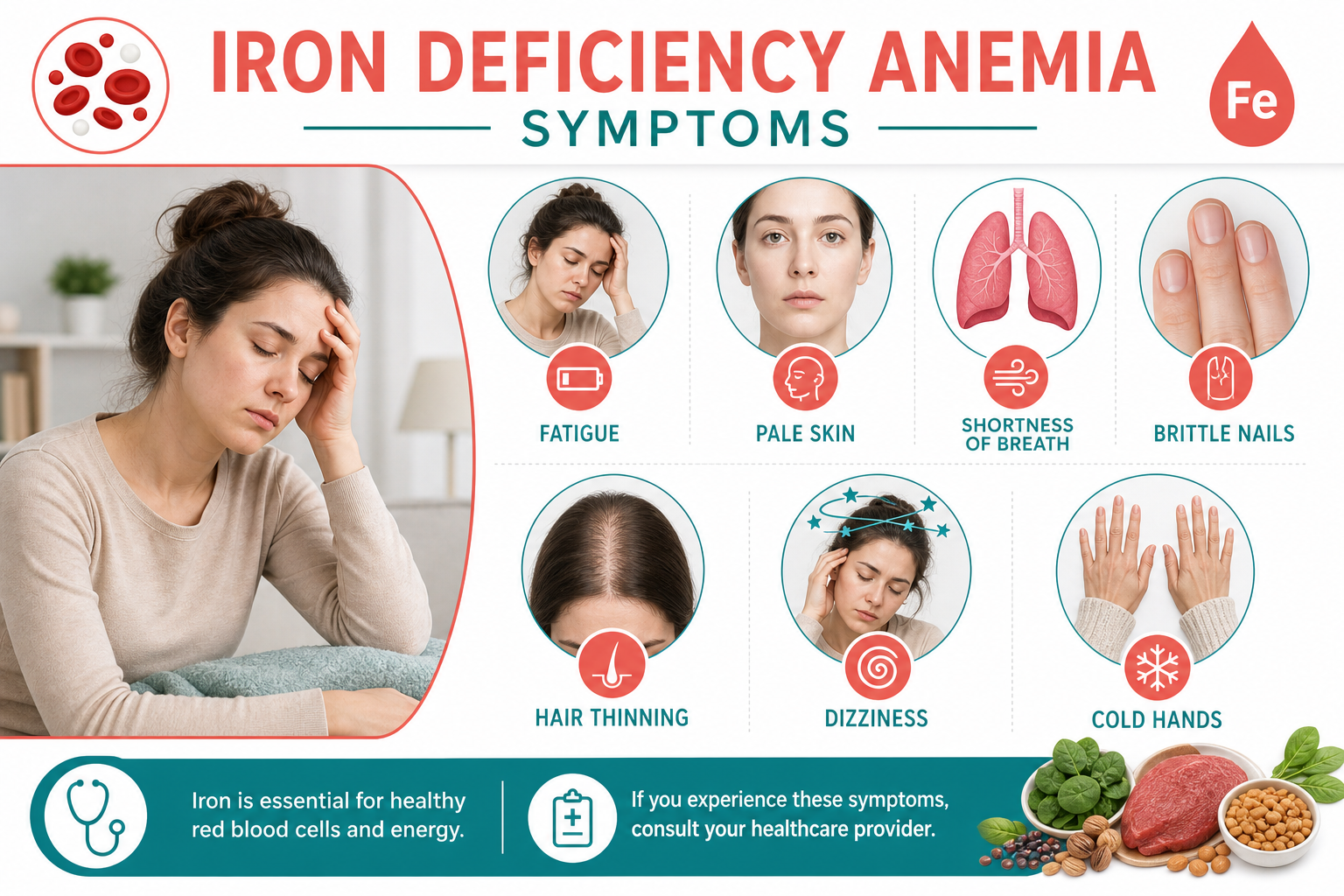
Early symptoms
- Unexplained fatigue — the hallmark symptom; similar to B12 fatigue and magnesium-related tiredness
- Weakness during normal daily activities
- Pale or dull skin — especially noticeable in face, nails, and inner eyelids
- Shortness of breath climbing stairs or exercising
- Headaches or dizziness — especially when standing quickly
- Cold hands and feet — poor circulation from reduced oxygen delivery
- Restless legs — uncomfortable urge to move legs at rest
- Cravings for ice, starch, or clay (pica) — a classic but underrecognized sign
Moderate to severe symptoms
- Rapid heartbeat or heart palpitations
- Chest pain with exertion (seek urgent care)
- Brittle or spoon-shaped nails (koilonychia)
- Hair thinning or increased shedding
- Poor concentration and brain fog
- Frequent infections
- Sore or swollen tongue (glossitis)
Symptoms in children
- Delayed growth or development
- Poor appetite
- Behavioral changes and learning difficulties
- Pale skin and irritability
Symptoms in pregnancy
Iron needs increase significantly during pregnancy. Untreated deficiency raises risks of preterm delivery, low birth weight, and postpartum anemia. Prenatal iron screening is standard in most prenatal care.
Causes of Iron Deficiency
Understanding the cause directs treatment — dietary changes alone will not fix ongoing blood loss.
1. Inadequate dietary intake
- Low intake of heme iron (meat, fish, poultry)
- Strict vegetarian or vegan diets without fortified foods or planning
- Chronic dieting or very low-calorie eating
- Over-reliance on processed foods low in minerals
Pair nutrition planning with our guides on folic acid foods and daily wellness habits.
2. Blood loss (most common cause in adults)
- Heavy menstrual periods (menorrhagia) — leading cause in premenopausal women
- Gastrointestinal bleeding from ulcers, polyps, hemorrhoids, or colorectal cancer
- Frequent blood donation without monitoring ferritin
- Internal bleeding from injury or surgery
- NSAID use (aspirin, ibuprofen) irritating the stomach lining
Red flag: Iron deficiency in men and postmenopausal women always warrants evaluation for hidden GI blood loss.
3. Increased iron needs
- Pregnancy and breastfeeding
- Rapid growth in infants and adolescents
- Endurance athletics increasing red blood cell turnover
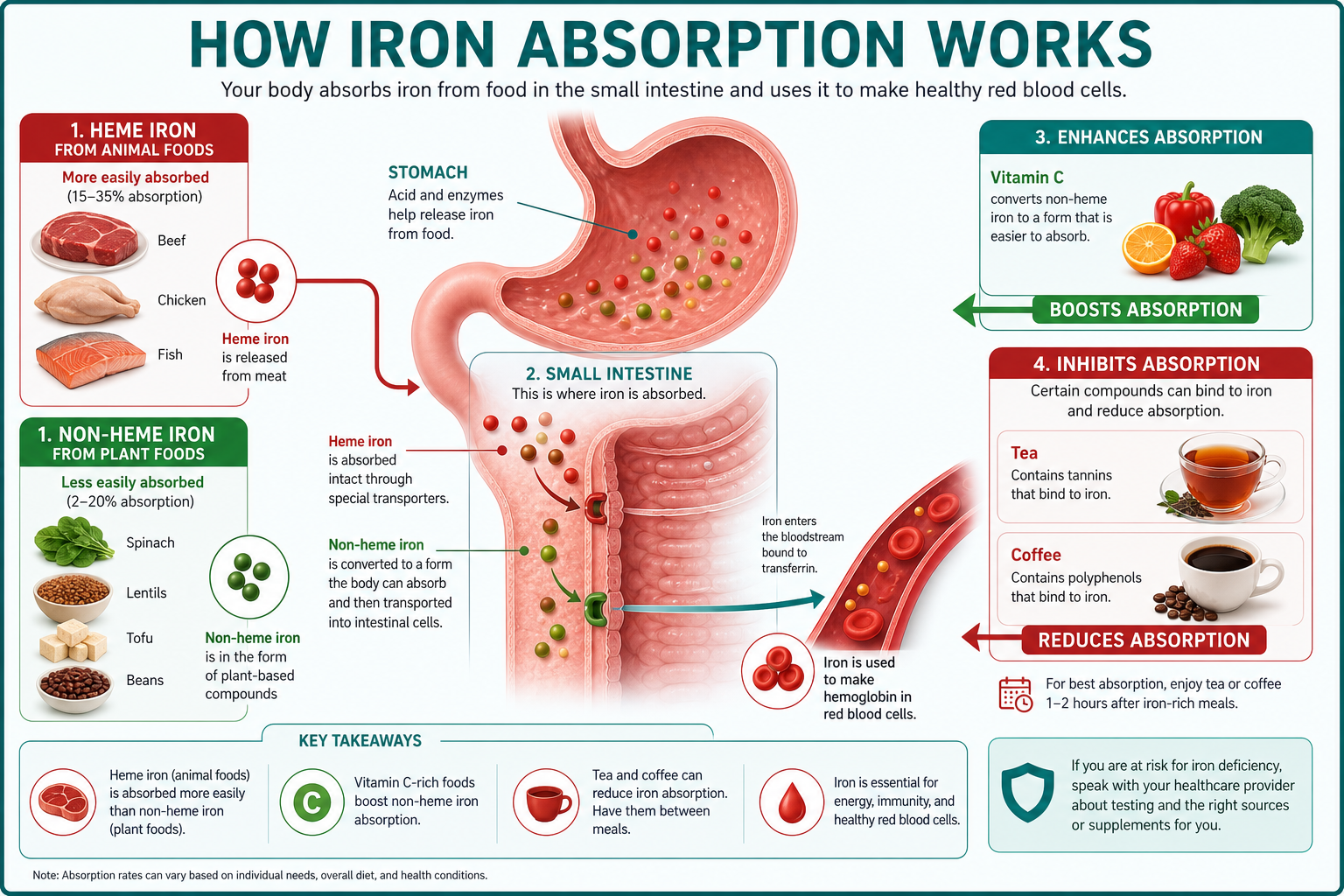
4. Poor absorption
Iron absorption occurs mainly in the duodenum. Conditions that impair absorption include:
- Celiac disease
- Inflammatory bowel disease (Crohn's, ulcerative colitis)
- H. pylori gastritis
- Bariatric surgery (gastric bypass, sleeve gastrectomy)
- Chronic digestive issues and malabsorption
If you have bloating, diarrhea, or unexplained weight loss alongside anemia, discuss gut evaluation with your clinician.
5. Medications and substances that block iron
- Proton pump inhibitors (PPIs) long-term
- Calcium supplements taken with iron-rich meals
- Tea and coffee polyphenols with meals
- High-dose zinc without balance
Who Is Most at Risk?
| Group | Primary risk factor |
|---|---|
| Menstruating women | Monthly blood loss |
| Pregnant people | Increased fetal and placental needs |
| Infants & toddlers | Rapid growth; cow's milk before age 1 linked to risk |
| Vegetarians/vegans | Lower heme iron intake |
| Endurance athletes | Foot-strike hemolysis and higher turnover |
| Frequent blood donors | Depleted ferritin stores |
| GI disease / post-bariatric | Malabsorption |
| Chronic kidney disease | Erythropoietin changes and treatment-related losses |
How Iron Deficiency Is Diagnosed
Do not diagnose anemia from symptoms alone. Standard workup includes:
Blood tests
| Test | What it shows |
|---|---|
| CBC (complete blood count) | Hemoglobin, hematocrit, MCV (cell size), RBC count |
| Ferritin | Iron stores — often the earliest marker to drop |
| Serum iron & TIBC | Current iron and binding capacity |
| Transferrin saturation | Percentage of transferrin carrying iron |
| Reticulocyte count | Whether bone marrow is responding |
Interpreting ferritin (general reference)
| Ferritin level | Typical interpretation |
|---|---|
| Below 15 ng/mL | Strongly suggests depleted stores |
| 15–30 ng/mL | Possible deficiency, especially with symptoms |
| 30–100 ng/mL | Usually adequate for most adults |
| Above 100 ng/mL | Normal stores (may be higher in inflammation) |
Ferritin is an acute phase reactant — levels can appear normal during infection or inflammation even when iron is functionally low. Your doctor interprets results in full clinical context.

Additional testing when needed
- Stool occult blood test or colonoscopy for GI bleeding
- Celiac serology
- Gynecologic evaluation for heavy periods
- Endoscopy for ulcer or gastritis
- B12 and folate levels (deficiencies often coexist)
Iron Deficiency Treatment
Treatment targets both replenishing iron and fixing the underlying cause.
1. Iron-rich diet

Heme iron sources (better absorbed):
| Food | Notes |
|---|---|
| Red meat (beef, lamb) | Highest bioavailability |
| Poultry (dark meat) | Moderate heme iron |
| Fish & shellfish (sardines, clams, oysters) | Excellent source |
| Liver | Very high iron — limit in pregnancy unless prescribed |
Non-heme iron sources (plant-based):
| Food | Absorption tip |
|---|---|
| Lentils, chickpeas, black beans | Pair with vitamin C |
| Tofu and tempeh | Choose calcium-set tofu mindfully with iron meals |
| Spinach and kale | Cooked greens offer more available iron |
| Pumpkin seeds & quinoa | Easy daily additions |
| Fortified cereals & bread | Check labels for iron content |
| Dried apricots & raisins | Snack with citrus |
Boost absorption:
- Add lemon, bell peppers, strawberries, or tomatoes to iron meals
- Cook in cast-iron cookware (small but meaningful boost)
Reduce blockers at iron meals:
- Avoid tea, coffee, and calcium supplements within 1–2 hours of iron-rich food or pills
- Separate high-calcium foods from iron-focused meals when possible
2. Oral iron supplements
Common forms:
- Ferrous sulfate — most prescribed; can cause GI side effects
- Ferrous gluconate or fumarate — sometimes better tolerated
- Iron bisglycinate — gentler on stomach; popular OTC option
Typical treatment duration: 3 to 6 months after hemoglobin normalizes to rebuild ferritin stores. Take on empty stomach if tolerated; with food if nausea occurs (accepting slightly reduced absorption).
Side effects: constipation, dark stools (normal), nausea, abdominal cramping. Increase fiber, fluids, and movement to manage constipation.
3. IV iron infusion
Used when oral iron fails, is not tolerated, malabsorption exists, or rapid correction is needed (e.g., late pregnancy, pre-surgery). Administered in clinical settings with monitoring.
4. Treat underlying blood loss
- Hormonal management or IUD for heavy periods
- Endoscopy/colonoscopy for GI sources
- Treat celiac, IBD, or H. pylori
- Adjust medications causing bleeding
Without fixing the source, anemia often returns after supplements stop.
Iron vs Other Nutrient Deficiencies
Many deficiencies share symptoms. Common overlap patterns:
| Nutrient | Overlapping symptoms | Link |
|---|---|---|
| Vitamin B12 | Fatigue, pale skin, anemia, neuropathy | B12 deficiency guide |
| Folic acid | Megaloblastic anemia, fatigue | Folic acid guide |
| Vitamin D | Fatigue, hair loss, muscle weakness | Vitamin D guide |
| Magnesium | Fatigue, cramps, weakness | Magnesium guide |
| Thyroid disease | Fatigue, hair loss, cold intolerance | Thyroid symptoms in women |
Doctors often check a nutritional panel when anemia is suspected rather than testing iron alone.
Prevention Tips
- Eat iron consistently — not just during flare-ups of fatigue
- Pair plant iron with vitamin C at most meals
- Monitor menstruation patterns — seek gynecologic care for heavy bleeding
- Screen during pregnancy — follow prenatal iron guidance
- Limit tea/coffee with meals if you are at risk
- Retest ferritin after treatment before stopping supplements
- Support overall health with hydration, sleep hygiene, and balanced wellness routines
When to See a Doctor — Red Flags
Seek urgent care for:
- Chest pain, fainting, or severe shortness of breath
- Rapid heartbeat with dizziness
- Black or bloody stools
- Signs of internal bleeding after injury
Schedule a routine appointment for:
- Fatigue lasting more than 2–3 weeks
- Hair loss with other anemia symptoms
- Heavy menstrual periods
- Unexplained iron deficiency in men or postmenopausal women
- Iron deficiency that does not improve with treatment
Also discuss screening if you have diabetes risk factors, high blood pressure, or chronic anxiety symptoms that may overlap with anemia-related fatigue.
Key Takeaways
- Iron deficiency anemia is the world's most common nutritional deficiency and a leading cause of chronic fatigue.
- Symptoms include tiredness, pale skin, breathlessness, hair thinning, brittle nails, and restless legs.
- Causes include blood loss (especially menstrual and GI), poor intake, malabsorption, and increased needs in pregnancy.
- Diagnosis requires blood tests — CBC and ferritin at minimum — not symptom guessing.
- Treatment combines iron-rich food, supplements when needed, and fixing the root cause of loss.
- Recovery takes weeks to months; retest before stopping supplements.
- Overlapping deficiencies with B12, folate, and vitamin D are common — comprehensive testing saves time.
Explore Related Guides
- Vitamin B12 Deficiency: Symptoms & Treatment
- Vitamin D Deficiency: Symptoms & Prevention
- Folic Acid Deficiency: Symptoms & Best Foods
- Magnesium Deficiency Symptoms & Treatment
- Thyroid Symptoms in Women
- Digestive Issues & Gut Health Guide
- Vitamin C Deficiency & Scurvy Signs
- Browse all Symptoms & Conditions articles
- Explore the full Health Articles hub
Medical Disclaimer
Symptoms Insight publishes general health information for educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified healthcare provider with questions about a medical condition, lab results, or supplement use.
About the publisher
Rajat
Health & Wellness Editor | Global
Health & Wellness Editor | Global
Rajat edits Symptoms Insight as a practical health publication focused on symptoms, vitamin deficiencies, skincare, wellness habits, and digital health — always encouraging readers to consult qualified healthcare professionals for personal medical decisions.
FAQ
Frequently asked questions
What are the most common iron deficiency symptoms?
Persistent fatigue, pale skin, shortness of breath, dizziness, brittle nails, hair thinning, headaches, and cold hands or feet are among the most reported symptoms. Many overlap with vitamin B12, vitamin D, and thyroid problems — blood tests help identify the cause.
What is the difference between iron deficiency and anemia?
Iron deficiency means body iron stores are low. Anemia means red blood cell count or hemoglobin is below normal. Iron deficiency often leads to iron deficiency anemia, but you can have low iron stores before full anemia develops.
How is iron deficiency anemia diagnosed?
Doctors typically order a complete blood count (CBC), ferritin, and sometimes iron studies and transferrin saturation. Ferritin below 30 ng/mL often suggests depleted stores, though optimal cutoffs vary by symptoms and guidelines.
Can iron deficiency cause hair loss?
Yes. Low iron is a well-known contributor to hair shedding and telogen effluvium, especially when deficiency is prolonged. Hair loss also occurs with thyroid disease, stress, and B12 deficiency — evaluation should check multiple causes.
Which foods are highest in iron?
Red meat, liver, shellfish, lentils, beans, tofu, spinach, pumpkin seeds, fortified cereals, and dried apricots are strong sources. Pair plant iron with vitamin C (citrus, peppers, tomatoes) to improve absorption.
Should I take an iron supplement?
Supplements help when diet alone cannot restore levels or when deficiency is confirmed, but they can cause constipation, nausea, and interact with medications. Never self-dose high iron without testing — excess iron is harmful.
Who is most at risk for iron deficiency?
Menstruating women, pregnant people, infants and young children, vegetarians without careful planning, endurance athletes, and people with chronic blood loss or malabsorption (celiac, IBD, bariatric surgery) are at highest risk.
How long does it take to recover from iron deficiency anemia?
Energy often improves within 2 to 4 weeks of treatment, but replenishing iron stores fully can take 3 to 6 months or longer depending on severity, cause, and whether underlying blood loss is treated.


